Recognise the consequences of PV and be ready to react
- Not all polycythaemia vera (PV) patients are the same-some are at increased risk of disease progression or thromboembolic events (TEs)[1]
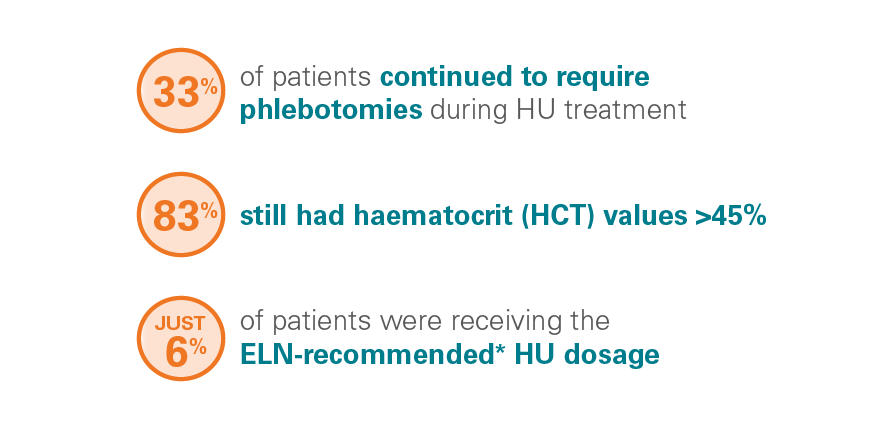
- Approximately 1/4 of patients with PV develop resistance/intolerance to hydroxyurea (HU) and the consequences can be life threatening[2]
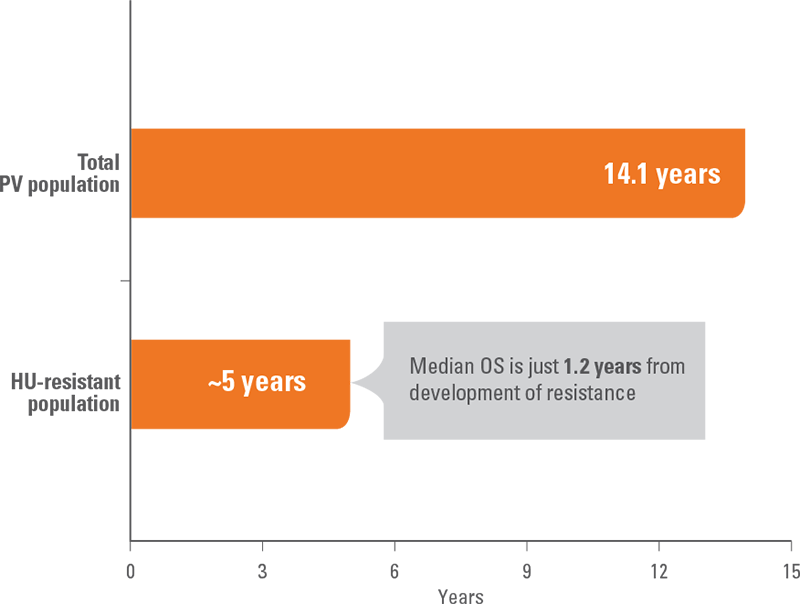
- HU-resistant patients have a median overall survival (OS) of 5 years, and just 1.2 years from development of resistance[3]
- TEs are observed in ~40% of patients with PV and may still occur in spite of treatment with HU[1],[4],[5]
- Only JAKAVI provides superior response, symptom control, and survival regardless of your patient’s HU resistance or intolerance status[6]-[9]
Polycythaemia vera is a life-threatening disease with serious consequences for patients[3],[10]
Median overall survival by PV subgroup
*Dosage of ≥2 grams of HU per day.
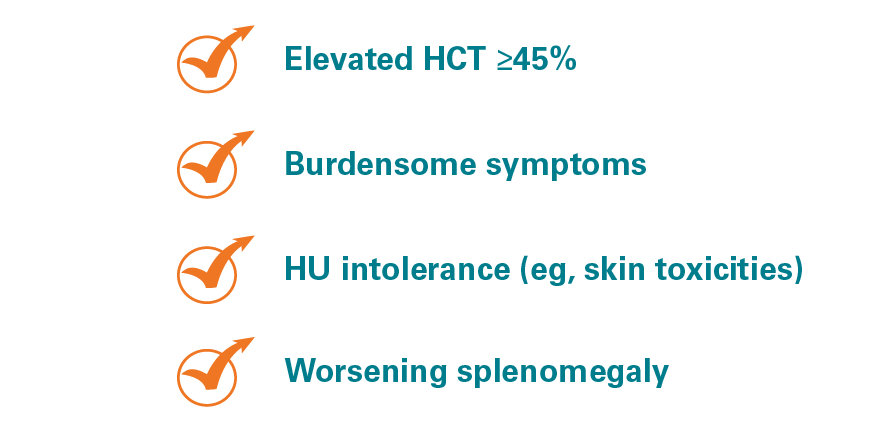
Know the signs of hydroxyurea resistance or intolerance so you can respond right away[3]
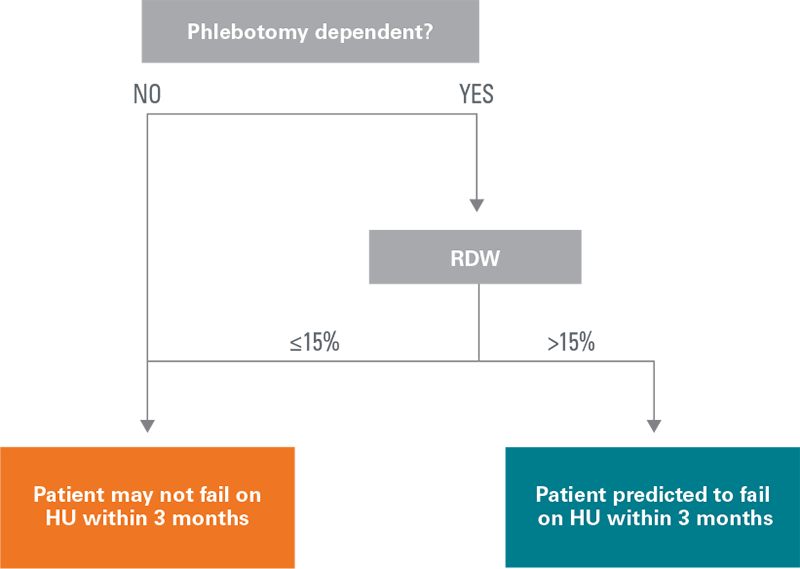
Are your patients at risk? Phlebotomy-dependent patients with an elevated red blood cell distribution width are predicted to fail* HU within 3 months[8]
Algorithm based on patients without a history of thrombosis
Results from a study evaluating the incidence of TEs in HU-treated patients with PV (median treatment duration, 27 months). The study used records from the US OPTUM database between 2007 and 2017. Machine learning was then used to build a precise and scientifically robust model to predict the occurrence of TEs in PV patients with/without a history of TEs and HU failure (defined by either ELN hematologic criteria or TEs).
ELN, European LeukemiaNet.
*Failure of HU was defined following haemotological ELN consensus criteria, excluding a dose of ≥2 g/day of HU, an insufficient reduction in splenomegaly, leg ulcers, or any other unacceptable HU-related toxicities.
†Arterial thrombosis was defined as myocardial infarction, transitory cerebral ischemic attack, acute cerebral ischemic stroke, or acute peripheral arterial occlusion. Venous thrombosis was defined as peripheral vein thrombosis or pulmonary embolism.
- Phlebotomy-dependent patients with an RDW >15% are predicted to fail on HU within 3 months[14]
- A retrospective study of newly diagnosed patents between 2001 and 2019 also demonstrated increased risk of TEs in patients with higher RDW[15]
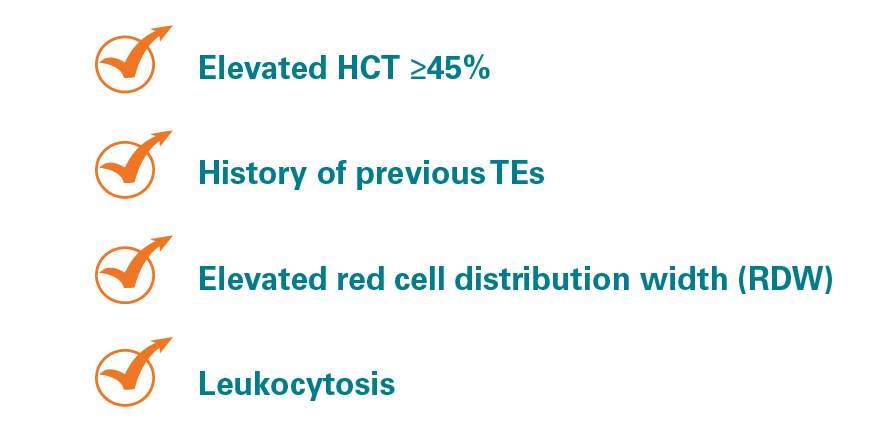
For patients with PV, thromboembolic events are a serious concern are you monitoring your patients for risk factors?
TE risk factors[1]:
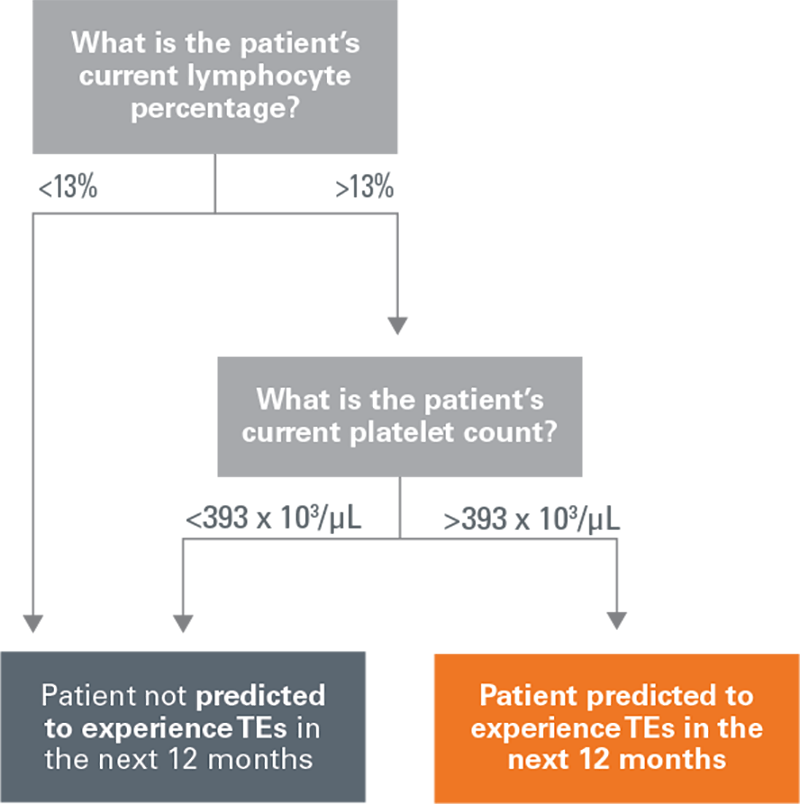
Elevated lymphocyte and platelet counts may predict a TE within 12 months[14]
PV patients with a history of TEs
Results from a study evaluating the incidence of TEs in HU-treated patients with PV (median treatment duration, 27 months). The study used records from the US OPTUM database between 2007 and 2017. Machine learning was then used to build a precise and scientifically robust model to predict the occurrence of TEs in PV patients with/without a history of TEs and HU failure (defined by either ELN hematologic criteria or TEs).
- In this machine-learning analysis of real-world data, patients with a history of TEs who have lymphocyte percentage >13% and platelet counts >393 x 103/μL are at risk of another TE within 12 months[14]
- A retrospective study of newly diagnosed patients between 2001 and 2019 also demonstrated increased risk of TEs in patients with higher RDW[15]